
The SAHS:
- recognises that for the non-specialist, clinical guidelines are often complex and difficult to digest.
- has therefore developed an algorithm to assist the non-specialist in making relatively quick and easy diagnostic and management decisions.
- algorithm is available under the section on “GUIDELINES”.
However, BEFORE studying the algorithm, FIRST follow a summary of the processes (SEE 9 KEY QUESTIONS BELOW – CLICK TO ACCESS ANSWERS) that should be taken to make key diagnostic and management decisions.
These processes are derived from the SAHS guidelines (2012) and other hypertension guidelines.
- For questions which are not listed below, please refer to the SAHS guidelines.
A word of caution.
This web-page is for educational purposes ONLY and is NOT intended to be a substitute for the advice of appropriate health care professionals or for independent research and judgement.
The SAHS does not accept responsibility or liability arising from any information contained in or any error of omission from the protocol or from the use of any information contained herein.
1. What is the most correct method of measuring blood pressure?
a) Patient should be in the sitting position with their back supported, arm bare and resting on a surface at heart level, for at least 5 minutes before measurement.
b) It is preferable that patients should not have smoked, ingested caffeine-containing beverages or had food in the previous 30 minutes.
c) An appropriate sized cuff should be used.
- Standard cuff (12 cm) for a normal arm
- A larger cuff (15 cm) for an arm with a mid-upper circumference> 33 cm
(ie. the bladder within the cuff should encircle 80% of the arm)
Inappropriate sized cuffs may lead to overestimation (if cuff too small) or underestimation (if cuff too large) of BP by as much as 20-30 mm Hg.
d) Both systolic BP (SBP) and diastolic BP (DBP) should be recorded. At the initial consultation BP should be measured in both arms, and if there is any discrepancy it should be measured thereafter in the arm with the higher BP. The SBP should be first estimated by palpation to avoid missing the auscultatory gap. SBP is measured at the first appearance of sound (phase 1) and DBP is measured at the disappearance of the sounds (phase V).
e) The BP recorded should be the average of 2 readings taken 1 minute apart. If the first 2 readings differ by > 5 mm Hg, additional readings should be taken.
2. What is an abnormal blood pressure?
- SBP/DBP ≥ 140/90 mm Hg
3. How often should the measurement be made before a diagnosis is made?
- Repeat measurementS should be performed on 3 separate occasions when either the initial SBP is between 140 and 160 mmHg or the DBP is between 90 and 100 mmHg. These 3 separate occasions should occur within 2 months to determine if the patient should be diagnosed as hypertensive.
- If SBP/DBP is ≥ 160/100 mm Hg then further measurements are NOT required, as the patient HAS hypertension.
4. Which measurement devices can I use?
- A mercury sphygmomanometer which is not worn-out by overuse is the most accurate measurement approach, but may be phased out with time because of the hazards related to mercury.
- As long as they are regularly serviced, anaeroid manometers and automatic BP monitors may be used.
- An up-to-date list of validated automatic devices can be found on various independent websites (eg. http://www.dableducational.org/ or http://bhsoc.org/Blood_pressure_list.stm) - see section on “BP DEVICES”.
5. Should I exclude treatable secondary causes of hypertension?
- Most cases of hypertension are from primary causes.
-
However, obvious secondary causes should be excluded by identifying typical clinical symptoms and signs of:
- Hypo- or hyperthyroidism
- Cushing’s syndrome or disease
- Phaeochromocytoma
- Coarctation of the aorta
- Renal artery stenosis
- Polycystic kidney disease
- Acromegaly
- Liver disease
- In addition patients should be asked about oral contraceptive use and pregnancy.
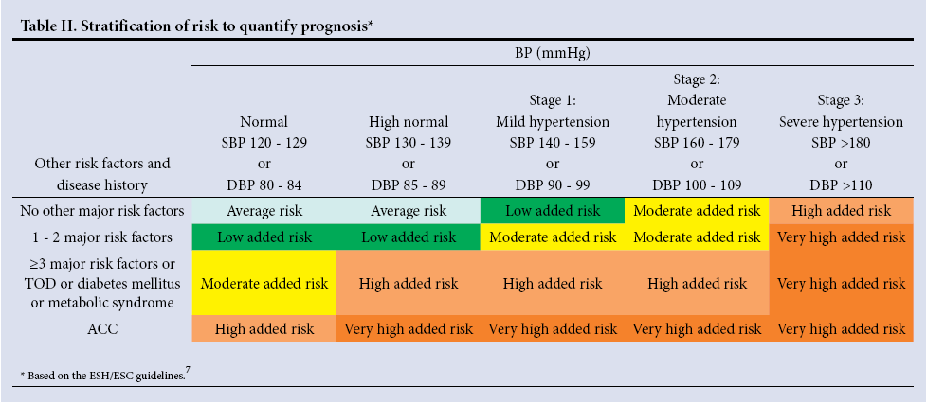
- In order to make management decisions (see Question 5 below), you should first cardiovascular ‘risk stratify’ your patient according to Table II from the SAHS guidelines (see below).
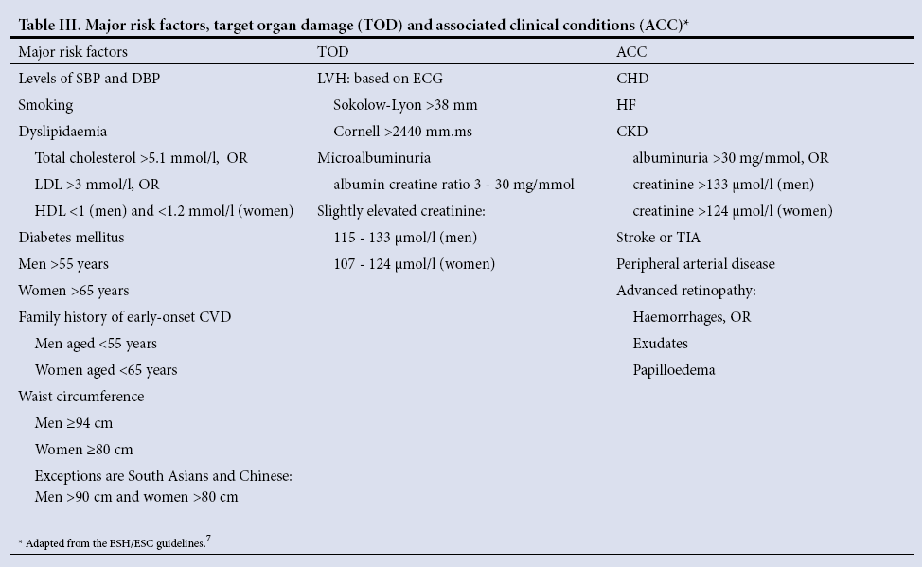
- To do this you need to account for major cardiovascular risk factors and the presence of target organ changes (see Table III from the SAHS guidelines, below).
-
Importantly, you are referred to the SAHS and other guidelines (see section on “Guidelines” regarding the:
- use of body mass index or waist-to-hip ratio, rather than waist circumference, to ‘risk stratify’
- importance of the metabolic syndrome.
Seedat and Rayner. S Afr Med Journal 2012;102:57-84.
Seedat and Rayner. S Afr Med Journal 2012;102:57-84.
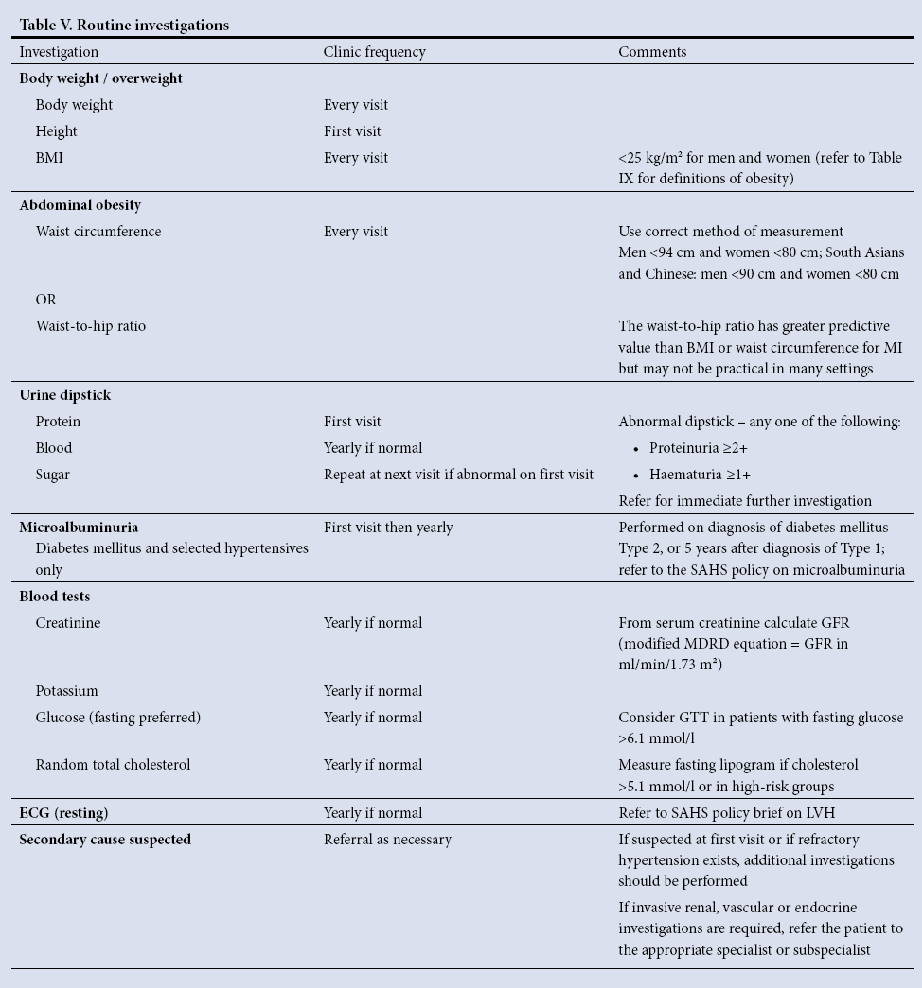
- To assess the level of cardiovascular risk, a number of investigations are required.
- To exclude renal failure as a secondary cause of hypertension, measurements of renal function are required. Table V from the SAHS guidelines (see below) lists the recommended routine basic investigations.
- Apart from measurements of overweight and obesity, the tests are performed annually unless the results are abnormal.
- Abnormal or suspicious results must be repeated as clinically indicated.
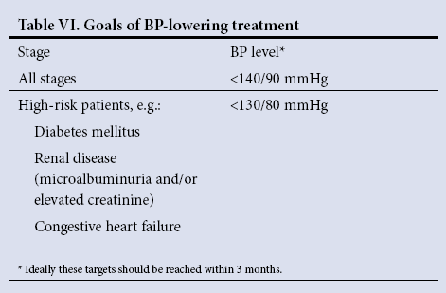
The target BP levels vary according to associated clinical conditions as shown in Table VI from the SAHS guidelines (see below).
Seedat and Rayner. S Afr Med Journal 2012;102:57-84.
Importantly:
- It is now contentious as to whether BP should be lowered in diabetes mellitus to these values.
- If renal disease co-exists however, current thinking is that the lower BP thresholds should be achieved.
These issues are discussed in the reappraisal of the European Society of Hypertension guidelines
(Mancia et al. J Hypertens 2009;27:2121-2158 see section on “EXPERT OPINIONS”).
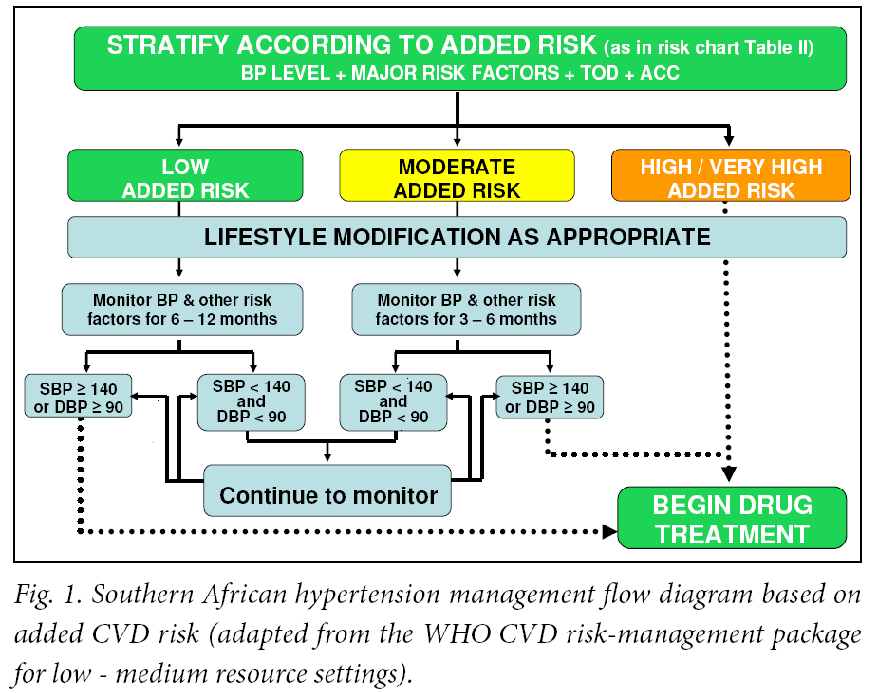
Figure 1 from the SAHS guidelines (see below) shows the approach to managing patients with an increased BP, who fall into the different risk categories of hypertension.
- Patients in the high/very high added risk categories require immediate drug therapy together with lifestyle management.
- Patients in other categories a 6-12 month trial of lifestyle management should be considered before drug therapy is instituted.
Seedat and Rayner. S Afr Med Journal 2012;102:57-84.
a) Achieve and maintain ideal weight with a body mass index between 18.5 and 24.9 kg/m2.
For weight loss refer to the two local guidelines for the prevention and management of obesity
(see section on “Guidelines”.
b) Limit total sodium intake by:
- Removing the salt cellar from the table
-
Reducing the intake of the following foods:
- packet soups; stock cubes; gravies; processed cheese; many breakfast cereals; bread; salty snacks; tinned food; ham; bacon; tongue; corned beef and salami.
- Gradually reducing added salt in food preparations.
Salt intake should be limited to < 2 400 mg/day by consuming < 1 teaspoon of salt per day.
Inform patients that:
- Food may taste bland initially, and encourage the use of lemon juice, herbs and spices as alternative seasoning.
- Taste adaptation to reduced sodium intake occurs with time.
- Food labels list salt content as sodium.
- Sodium-free means < 5 mg per 100 g serving
- Very low sodium means up to 40 mg per 100 g serving
- Low sodium means up to 120 mg per 100 g serving.
c) Limit alcohol intake to:
- 2 standard drinks per day for men.
- 1 standard drink per day for women and small men.
A standard drink contains about 10 g of ethanol (e.g. 25 ml spirits, 125 ml wine, 340 ml beer, 60 ml sherry, 25 ml liqueur).
d) Advise a diet:
- which is low in total fat
- with high intake of fruit and vegetables (5 portions per day)
- containing regular use of low-fat dairy products
- with high intake of high-fibre whole-grain foods
- containing fish rather than red meat
- containing products low in saturated fat
- with sparing use of sugar and sugar-containing foods.
e) Avoid intake of beverages with high caffeine levels, but the modest use (1 - 2 cups per day) of coffee will not increase BP.
f) Advise regular moderate-intensity exercise for at least 30 minutes on most or preferably all days of the week.
- Moderate levels of exercise can be achieved by brisk walking and should be 50 - 70% of peak oxygen consumption (V02peak) which is equivalent to 65 – 75% of maximum HR (maximum HR can be estimated by 220 - age).
- Exercise bouts can either be continuous or accumulated in shorter time periods throughout the day.
- The benefit of exercise is dose-response related, and the early adaptations from a sedentary lifestyle to becoming moderately active have the greatest effect.
- Patients with uncontrolled hypertension should embark on exercise training only after evaluation and initiation of therapy.
g) Stop the use of all tobacco products.
- The use of snuff is common among South African women who traditionally do not smoke tobacco.
- Nicotine replacement therapy should be used for patients with hypertension while under medical supervision.
Once the decision to institute drug therapy has been taken (see answer to Question 5), there are three important classes of antihypertensive agents for the management of persons without indications:
- diuretics (thiazide-like and thiazide)
- angiotensin-converting enzyme inhibitors (ACE-I’s)
- calcium channel blockers (CCBs)
There is presently controversy around the use of some beta-blockers (atenolol), but others may be safe.
The following approach is currently part of the SAHS guidelines (see section on “Guidelines”):
- Start ONE agent if BP<20/10 mm Hg above target BP
- Start TWO agents (fixed drug combinations) if BP ≥20/10 mm Hg above target BP
If one follows an initial monotherapy approach, the SAHS recommends ONE of the following:
(i) Low-dose hydrochlorothiazide (12.5 mg preferred up to maximum 25 mg) or thiazide-like diuretic as initial therapy. Higher diuretic doses are not recommended because of the risk of new diabetes.
- Where there are no other indications, ONE of the aforementioned agents NOT already given should be used as an add-on agent.
(ii) ACE-I [in ACE-I intolerance use angiotensin II receptor blockers (ARBs)].
(iii) CCB long-acting dihydropyridines or non-dihydropyridines.
- If BP is still not controlled to target levels, then add the third agent listed above and NOT already administered.
Do not replace one drug for another, unless the reason for replacement is that the initial medication
caused side-effects.
Where appropriate use fixed-dose combinations.
It is crucial to ensure that the patient understands the importance of returning drug containers and unused drugs.
Continued monitoring and management of drug side-effects is essential.
Table VIII from the SAHS guidelines (see below) lists the clinical considerations (indications) for the major drug groups when selecting antihypertensive drug therapy.
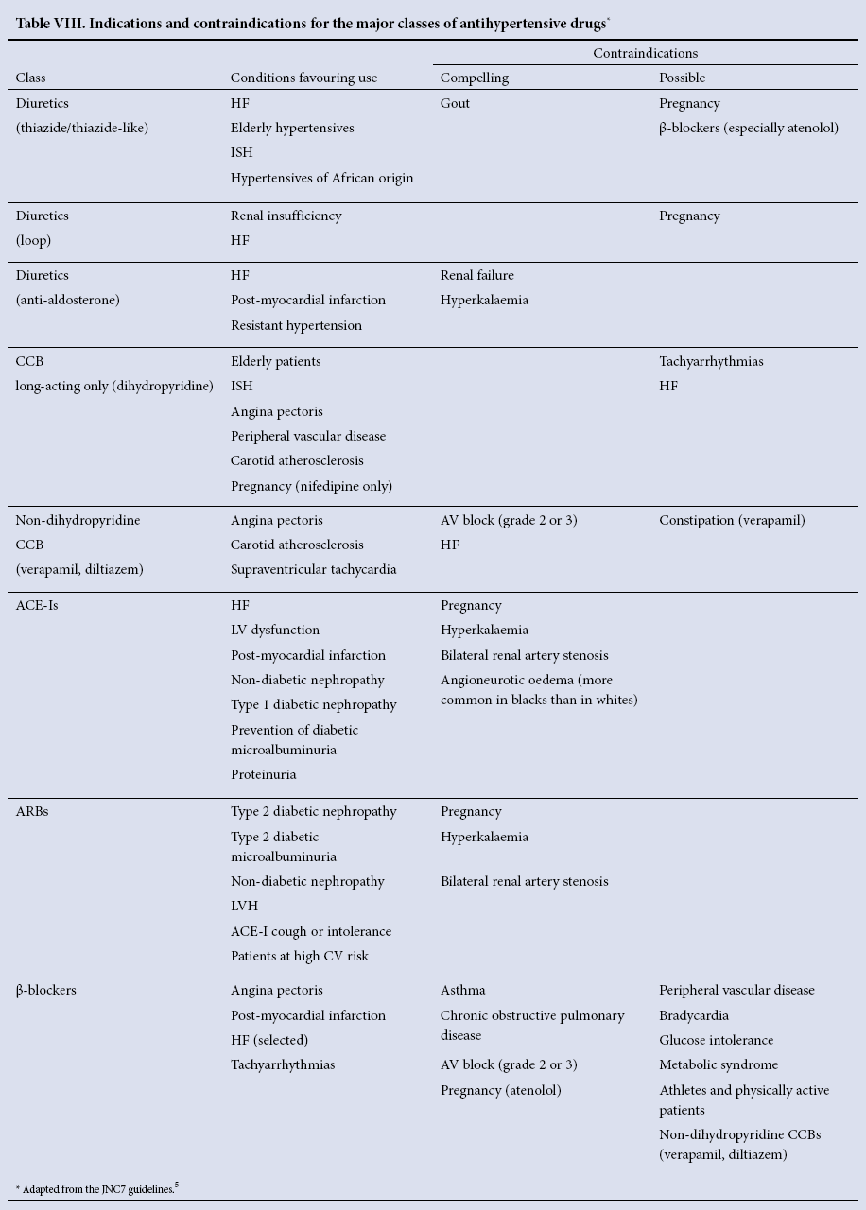
Seedat and Rayner. S Afr Med Journal 2012;102:57-84.
- Patients with severe hypertension (stage 3 DBP > 110 mmHg and / or SBP > 180 mmHg) may fall into one of three categories (see below) which determine the urgency of their treatment.
- Patients should be managed or referred to the appropriate level of care and caregiver in accordance with local protocols.
- Sustained severe hypertension requires immediate drug therapy, and lifestyle modification must be followed as soon as possible.
Category 1: Asymptomatic Severe Hypertension
- If asymptomatic, keep the patient in the care setting.
- Repeat BP measurement after resting for 1 hour.
-
If the second measurement is still elevated to the same level:
- start oral therapy using 2 drugs together.
- one of the drugs should be a low-dose thiazide-like diuretic.
- the other drug is usually a dihydropyridine CCB.
- Follow up within a week or earlier, escalating treatment if needed.
- Early referral is advised if BP is not controlled within 2 - 4 weeks
Category 2: Hypertensive Urgency*
-
This level of hypertension is symptomatic, usually with:
- severe headache or shortness of breath and oedema.
- There are no immediate life-threatening neurological, renal, eye or cardiac complications such as are seen in the hypertensive emergencies.
- Ideally, all patients with a hypertensive urgency should be treated in hospital by experienced staff.
Category 3: Hypertensive Emergency*
- A hypertensive emergency exists when acute elevation of BP is associated with acute and ongoing organ damage to the kidneys (renal failure), brain (stroke), heart (myocardial infarction or heart failure), eyes (grade 3 or 4 retinopathy) or vascular system (ruptured aortic aneurysm, threatened limb, etc).
- These patients need rapid (within minutes to a few hours) lowering of BP to safe levels.
- Once a patient is identified as having a genuine hypertensive emergency, immediate hospitalisation is essential in an intensive care unit with experienced staff and modern facilities.
* For details of in hospital care, please see SAHS guidelines in the section on “Guidelines”.

